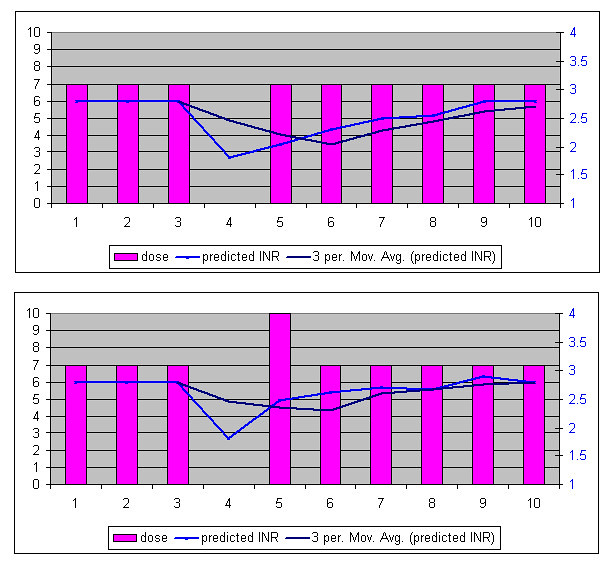
Oh, and PEM, this model (used in a spreadsheet) will give you an approximation of what will be happening to the warfarin in your system.
Make C2 your warfarin dose, fill this down for the series of C
In Colum D
start with this series and continue
=C2
=D2+0.75*C2
=C4+(0.75*C3)+(0.5*C2)
=C5+(0.75*C4)+(0.5*C3)+(0.3*C2)
=C6+(0.75*C5)+(0.5*C4)+(0.3*C3)+(0.25*C2)
after here you can fill down
NOTE: this model does not take into account actual metabolism NOR the actual bioavailability of the dose (which varies from person to person depending on their metabolism).
However it does provide a simple working model for you to undertake a little what if analysis on "what if I miss a dose". Especially when you factor in the rate of drop of INR observed in my above chart to estimate the biological response to a missing dose you can get a feel for the reaction of the system (your bodys system) to the changes.
This is of course a SIMPLE model, however my experience in modelling suggests that more complex models while potentially producing more accurate results can vary more wildly when the input parameters are in error. Essentially the less parameters the lower the accuracy but the lower the tendency for wildy inaccurate results too.
That's great - thanks! I'll try it out and line it up with my actual INR response to the recent coumadin dosages. I agree with your opinion about more parameters potentially increasing the model's sensitivity to variance - I haven't examined that closely, but I get the same intuition.
Best,
pem
")