At what point does an amateur (however well-informed) disagree with the expert?
Well the surgical guidelines are there to read. If the surgeon is not recommending following the guidelines then the surgeon is offering an opinion and should justify why with sound evidence.
If the amateur has been informed of the options then that's where the word "
consent" comes into "
informed consent"
Remember, do not confuse the capacity of the surgeon and skills with their being a human with biases. So this is why informed patient consent is key. Further don't down play the capacity of people on this forum to have a very good set of well recognised informational sources and personal experiences.
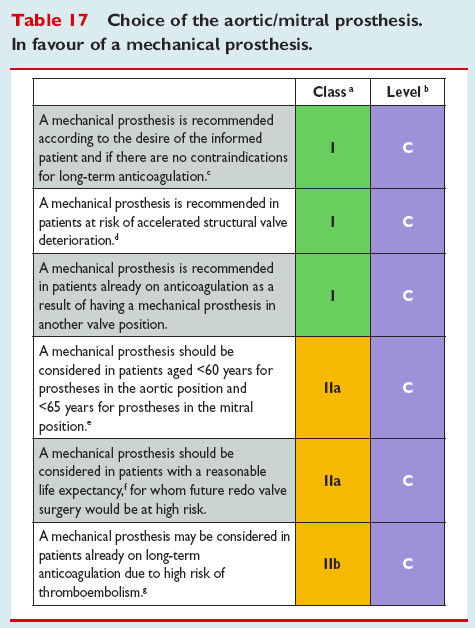
So lets first look at the guidelines (these are not current but current hasn't changed much)
1
the second last point is interesting, for if you pick a bioprosthesis and have the 'vision' of getting a TAVR later make sure you do your sums on what is a reasonable life expectancy for your age and then ask yourself this: "
would you be then in the position of being at high risk patient when you've reached the inevitable end of the bioprosthesis then valve in valve TAVR Structural Valve Degradation (SVD) road?"
worth pondering that.
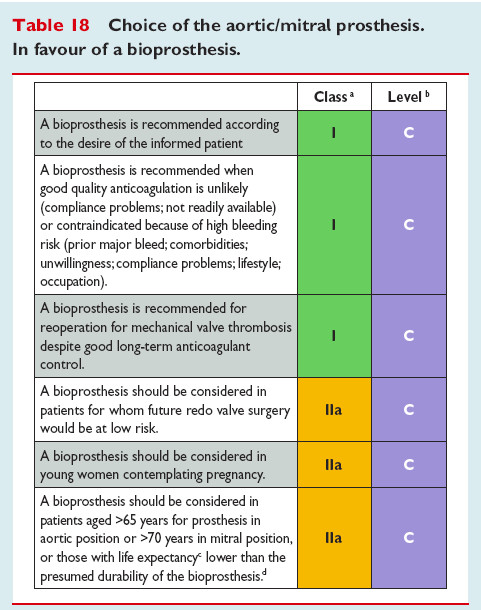
2
read those carefully and I would personally ask why they are ordered like they are.
Next lets look at this article:
https://www.ahajournals.org/doi/10.1161/JAHA.120.018506
note what that is and who publishes it
Within that it they concern themselves with the degeneration of bioprosthetic valves. They make the case right up front that there are two choice stems: mechanical (MHV) or tissue (BHV)
the following quotes from that are telling (I'll bold those):
Valve replacement surgery is the first‐line therapy for patients with valvular heart disease. In such treatment modality, a dysfunctional native valve is replaced by an artificial one, which can be a mechanical heart valve (MHV) or a bioprosthetic heart valve (BHV). MHVs are made of pyrolytic carbon, various polymers, and metal alloys, whereas BHVs represent valve substitutes that can be of 3 types: (1) chemically stabilized tissues of animal origin (xenografts), (2) valves obtained from cadavers or live donors during heart transplantation (homografts), or (3) patients' own valves (autografts) transplanted from one position to another. Both MHVs and BHVs have their advantages and disadvantages.
1,
2,
3 MHVs are durable yet highly thrombogenic, which necessitates life‐long use of anticoagulants. In contrast, BHVs do not require anticoagulant therapy and demonstrate excellent hemodynamic properties similar to those of native valves;
nonetheless, their durability is limited because of inevitable structural valve degeneration (SVD), a dangerous condition eventually requiring redo valve replacement, a major surgical intervention.
4,
5
SVD is an irreversible process
then:
Cyclic Loading as a Major Determinant of BHV Mechanical Degeneration
In heart valves, hemodynamic load is of cyclic nature. On average, native
valves undergo ≈600 million cycles of opening and closing during 15 years of operation and ≈3 billion cycles during a lifetime.
43 Cyclic stress, derived from the combination of stretching, flexure, and shear, may inflict delamination of the leaflets, leading to calcification and eventually resulting in valve failure.
short view: leather wears out
Throughout that article they make points like:
The durability of both xenografts and homografts also depends on host factors. For example, young age of graft recipient is one of the most significant risk factors determining early SVD onset, whereas patients >60 years of age often do not outlive the durability of BHVs because of relatively low life expectancy after valve surgery.
remember these are not "MY OPINIONS" they are those of THE ACCREDITED EXPERTS in the field. I just happen to have been informed by them.
So when someone here (usually older with a vested interest in a bioprosthetic) says "
we're all just patients" or "
nobody here is a doctor*" it is intended to discredit person presenting evidence they found informative ... this is also known as "shoot the messenger". I can only think their reason is to put more people on "their team"
Frankly I've been on both teams and I don't care nor will it effect me which team you pick. My responsibility (to myself having been through this and having been young and still not yet 60) is to present information to you to assist your process of becoming "an informed patient"
Best Wishes
*(not to mention some of us here ARE doctors)



")