Good morning (from Australia)
appropriate concern .... but first let me take a step back to your earlier comment about the views of the surgeon.
My present thinking on that is that surgeons have to think statistically, for they don't know you. They specalise in Surgery not post surgical management. They genuinely don't see past 10 years because statistically that's fraught. If you look through my blog post here
http://cjeastwd.blogspot.com/2014/01/heart-valve-information-for-choices.html
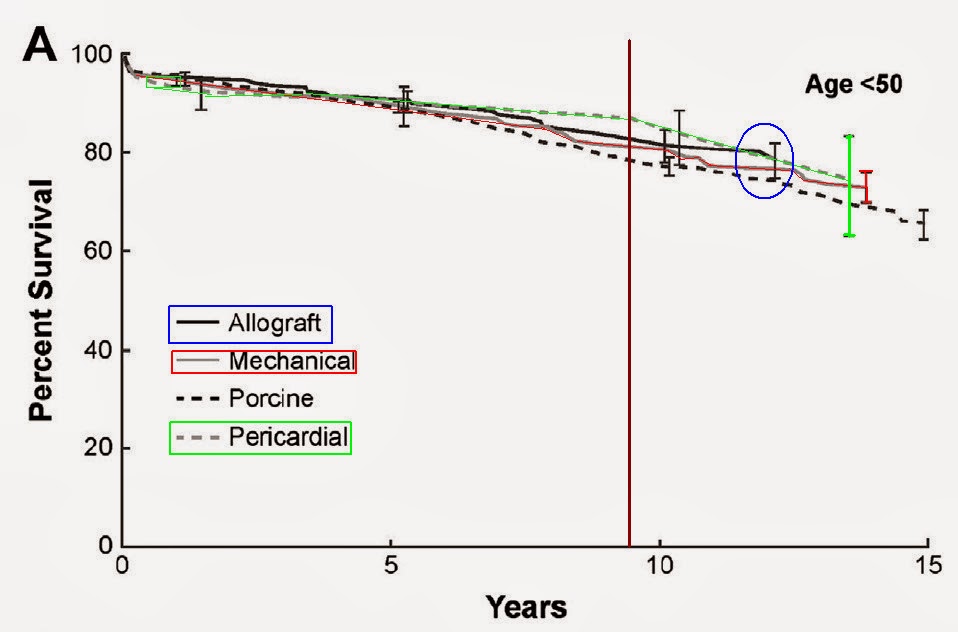
you'll see some graphs like this one:
Note the years on that scale.
This is not unusual, and as you begin your research into what to do next (which should be a casual affair because you should have about a decade to need to do anything about it) you'll begin to see a pattern: Bio-prosthetic valves last longest in the oldest, who (because of age) statistically don't need the valve to last beyond 15 years.
I'm currently 57 and 15 years is on the edge of where I may live to. Back when I was 47 that would see me being concerned about this before I get to 67.
So I see your point.
Getting back to surgeons and thinking statistically, they know the stats on the surface like the back of their hand: things often don't go well for mech-valvers for the primary reason of drug compliance (
they don't friggin take it) and crappy INR management (
putting them at risk of harm from bleed events or clotting events. I'll come back to that).
Accordingly they look at the data surface (because digging into the psychology and mechanisms of change in INR management clinics) is not their speciality.
It can however become the patients speciality if they so choose. Personally I take my health seriously and as I once put lots of effort into things like exersize, diet, safety (at work and in recreation) I now put effort into INR management. You'll see that mentioned in that blog post too.
What we don't know so well is what the age distribution of that set of "incidents" is (
because the stats choose not to present it and because there are statistically so few under 50yo patients managing INR let alone self managing INR) ... although we do now know the INR distributions of that. This graph shows where the danger areas are:
View attachment 888106
and its well known that keeping inside that green zone that you have about the "normal" level of risk.
That is the nub of the matter pure and simple: keep in the green and get a valve that will never fail and you can minimise the requirement for reoperation.
Your situation is complicated by the situation you are in and so you are not making that choice (yet).
As I see it you need to gradually and carefully evaluate the risks of the various choices which are before you. Your options of TAVR may or may not pan out as described (for many reasons, not least of which may be your own situation at that time). By that (hopefully distant) time you will have acquired the knowledge you need to make a decision which you are comfortable with on what to do then.
hope that helps