I have on rare occasions missed taking my warfarin for one day. Typically, when I realize this, I just pick up and take my normal dose and get on with things. Normally I take my warfarin in the evening with dinner. Once or twice I took an extra half dose the next morning after resuming my normal dose the evening before, but it has not made much difference in time to get back to normal INR range.
This evening (Monday), however, when I went to take my warfarin dose, I saw that the pills for Saturday and Sunday were still in their little compartments of my pill minder. So now, for the first time, I have missed two consecutive days of my warfarin dose. Comments regarding the "Forgotten Weekend" are deserved.
I took 1.25 times my normal dose this evening. My plan is to take an extra half-dose tomorrow morning (about 14 hours after my normal dose. Then, I plan to resume my normal dose tomorrow (Tuesday) evening.
I will test my INR tomorrow evening again when I take my pills, and if I am still below 2.0 I will take another "extra" 1/4 dose Tuesday evening followed by another 1/2 dose Wednesday morning.
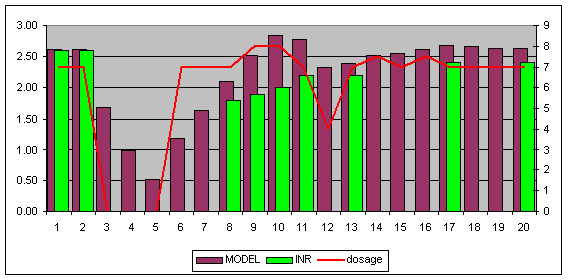
I thought that this would be an interesting opportunity to test Pellicle's spreadsheet model of what the optimum strategy should be to return to within range in the shortest time, without risk of serious overshooting, based on his model's prediction.
I home test, and fortunately, I took my INR reading Saturday morning, just prior to the time I missed the doses Sat & Sun evenings.
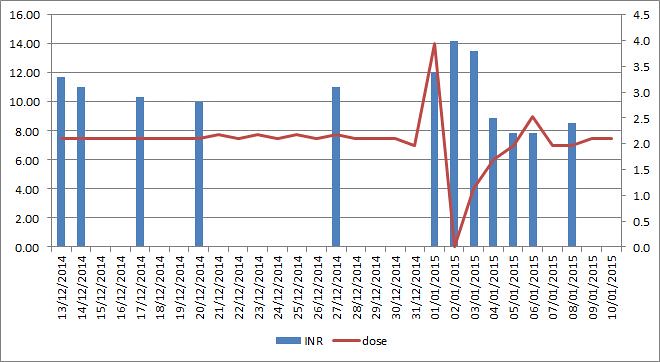
My range is 2.5-3.5 (target 3.0). On Saturday morning, my INR was 2.8.
Monday evening (just now) my INR is down to 1.5.
I take a lot of warfarin (12.5/day) and my INR drops like a rock when I miss a dose (or 2).
So, I'm curious to see if Pellicle's model would lead to a different predicted optimal recovery strategy than I have outlined above.
I look forward to the reply.
This evening (Monday), however, when I went to take my warfarin dose, I saw that the pills for Saturday and Sunday were still in their little compartments of my pill minder. So now, for the first time, I have missed two consecutive days of my warfarin dose. Comments regarding the "Forgotten Weekend" are deserved.
I took 1.25 times my normal dose this evening. My plan is to take an extra half-dose tomorrow morning (about 14 hours after my normal dose. Then, I plan to resume my normal dose tomorrow (Tuesday) evening.
I will test my INR tomorrow evening again when I take my pills, and if I am still below 2.0 I will take another "extra" 1/4 dose Tuesday evening followed by another 1/2 dose Wednesday morning.
I thought that this would be an interesting opportunity to test Pellicle's spreadsheet model of what the optimum strategy should be to return to within range in the shortest time, without risk of serious overshooting, based on his model's prediction.
I home test, and fortunately, I took my INR reading Saturday morning, just prior to the time I missed the doses Sat & Sun evenings.
My range is 2.5-3.5 (target 3.0). On Saturday morning, my INR was 2.8.
Monday evening (just now) my INR is down to 1.5.
I take a lot of warfarin (12.5/day) and my INR drops like a rock when I miss a dose (or 2).
So, I'm curious to see if Pellicle's model would lead to a different predicted optimal recovery strategy than I have outlined above.
I look forward to the reply.
")