I've intentionally (and once accidentally) lowered my INR for a procedure - somewhere around 1.5 or so -- and chose not to bridge with Lovenox. I just returned to my regular daily dose and in 3 days, my INR was back to normal. A few days below range shouldn't hurt you.and @LoveMyBraveHeart
to suppliment this:
- INR is indeed a rubbery figure, almost devoid of precision (not least by its very definition of "averages and normalised" but also because of the issues in surrounding
- The goal of the process is to avoid a stoke and minimise bleeding (and bleeding exacerbated injuries), not a "score" Accordingly I would point you to this chart summarising outcomes
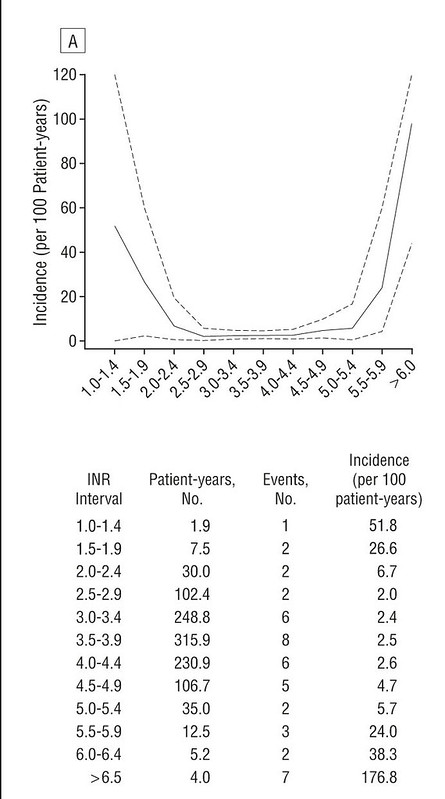
from "Optimal level of oral anticoagulant therapy for the prevention of arterial thrombosis in patients with mechanical heart valve prostheses, atrial fibrillation, or myocardial infarction: a prospective study of 4202 patients." (and I'd say over four thousand is a significant number)
https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/415179
Some may argue that as the study approaches 10 years old that its "out of date" however I'd counter that
So ultimately you may feel that your valve allows you to remain safe at a lower INR level, and in some cases that's actually a maker specific claim. However if you do wish to go lower (for what possible benefit I can't be sure) then make sure you strictly adhere to the makers notes on that protocol for the long term.
- there has been no significant change in human metabolism
- warfarin remains unchanged as the anticoagulant of reference
- there are no significant changes in Mechanical Valves (nor are there likely to be in the foreseeable future.
Ultimately I believe there is sufficient evidence to argue that INR ~ 1.4 is of no significant concern for the short term, but please do return to target promptly.
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Rules of ACT
- Thread starter pellicle
- Start date



Help Support Valve Replacement Forums:
This site may earn a commission from merchant affiliate
links, including eBay, Amazon, and others.
pellicle
Professional Dingbat, Guru and Merkintologist
only if they died from warfarin dose, which you are arguing doesn't kill them ;-)I guess that if you eat enough dead rats, it'll lower your INR, too.
#ISayThatsAJoke..
I didn't say that warfarin doesn't kill MOST rats -- it doesn't kill ALL rats. There are some strains that are resistant to Warfarin. It kills MOST rats.
pellicle
Professional Dingbat, Guru and Merkintologist
I didn't say that warfarin doesn't kill MOST rats ...It kills MOST rats.
Actually, it doesn't kill the ODD rat.
for reference, a nuance of Australian (and probably NZ) use of "odd" means that it gets at least one or two...
Probably its different in the USA
Agian
Well-known member
Odd also means 'strange'. A pipe-smoking hipster rat with a fedora might be considered quirky.
pellicle
Professional Dingbat, Guru and Merkintologist
agreed ... so does this mean a pipe-smoking hipster rat is unlikely to be killed by warfarin?Odd also means 'strange'. A pipe-smoking hipster rat with a fedora might be considered quirky.

perhaps a study is needed
")




$49.00
$62.95
Echocardiography: A Practical Guide for Reporting and Interpretation, Third Edition
Apex_media🍏

$27.99 ($0.23 / Count)
$34.99 ($0.29 / Count)
HerbaMe Heart Support and Blood Pressure Supplement, 120 Capsules, Promotes Cardiovascular Health, Healthy Cholesterol, Triglyceride, Homocysteine, CRP Levels | Natural Artery Cleanse and Protect
Global Pro Sales








$27.26 ($0.30 / Count)
$33.95 ($0.38 / Count)
Snap Supplements Heart Health Supplements and Blood Circulation Supplements, 90 Capsules
SnapSupplements





$28.91 ($0.32 / Count)
NutraPro Healthy Heart - Heart Health Supplements. Artery Cleanse & Protect. Supports Healthy Cholesterol and Triglyceride. GMP Certified
Gulliver Group


I used 'odd' as strange, rather than the numeric 'not even.' (1, 3, 5, 7, etc.).
Thinking about the word 'odd' we sometimes use an expression like 'a few odd' to mean 1 or 2 (or something). Again - in this case, I meant that there are some strange rodents that have developed an insensitivity to warfarin, and that aren't killed by a high dose.
Thinking about the word 'odd' we sometimes use an expression like 'a few odd' to mean 1 or 2 (or something). Again - in this case, I meant that there are some strange rodents that have developed an insensitivity to warfarin, and that aren't killed by a high dose.
pellicle
Professional Dingbat, Guru and Merkintologist
all good natured from this end ... so don't feel "oppressed" by any of this.we sometimes use an expression like 'a few odd' to mean 1 or 2 (or something). Again - in this case, I meant that there are some strange rodents that have developed an insensitivity to warfarin
I understand we call those rats "Super Rats" (as distinct from Politicians)
Agian
Well-known member
Pel, the rat you refer to looks suspiciously like Sherlock Holmes. He would not qualify as a hipster, given his vintage. A hipster rat eats deconstructed food and acts like a ******.
All good natured from here, too. No oppression felt or perceived.all good natured from this end ... so don't feel "oppressed" by any of this.
I understand we call those rats "Super Rats" (as distinct from Politicians)
Super Rats are probably somewhat predictable; politicians - not so much.
It's interesting to me to learn the differences in the languages that we all share. Now, I'll just jump under my bonnet and keep my head warm. (Or does bonnet mean hat down under? And, for that matter, do Australians and New Zealanders refer to North America as 'up over'? And if not, why not? Why shouldn't you be the center and the North Americans the 'other'?)
Thomas
Well-known member
Actually, it doesn't kill the ODD rat....
Does it kill "Normal" rats?
Sorry, couldn't resist.
Couldn't resist WHAT? The point was that normal rats are not immune to warfarin. It's only a few strains that have developed insensitivity to it.
pellicle
Professional Dingbat, Guru and Merkintologist
Even onesDoes it kill "Normal" rats?
Sorry, couldn't resist.