


Amy
Well-known member
- Joined
- Jan 6, 2013
- Messages
- 297
I was diagnosed with congenital severe aortic stenosis, at birth, I believe, and have been following it all this time, until Monday when the cardiologist noted a big jump in numbers and said "It's time." Current peak aortic valve gradient = 103.9 mmHg; mean = 63.3 mmHg. Two and a half years ago, when I last saw him, it was peak = 64 mmHg; mean = 41 mmHg. His words: "It's not an emergency, and it's not urgent, but you should have AVR surgery done in the next FEW WEEKS (!?) or at most few months, but before summer."
I have so many questions; and unfortunately am not confident my doctor either can or will answer them. I've learned a lot from the forum already, but now I want to ask a few more specific questions:
1. I went in because I had had chest pain that woke me up from sleep for 5-6 nights in a row. The cardiologist at first said he didn't think it was related to my AS; after viewing the echo he said he thought it WAS... Has anyone else had this? Did it end up being an indication that things were much worse than you thought? (trying to avoid that sudden death thing)
2. I usually deny any symptoms on exertion, (and symptoms at rest that I'd report were always dismissed by cardiologists) though I now think my exercise tolerance must have gradually gotten worse, and with that, shortness of breath walking up hills, etc. With turning 40 I maybe also thought I was just getting old or out of shape... But now I've been told it's time for surgery, that things have progressed/gone downhill, I feel every single pain, ache, twinge and arrhythmia in my heart; along with every episode of gasping for a breath, even at (particularly at) rest. If they are from the AS (which I more and more suspect they must be) - how bad of a sign is this? Would wearing a Holter for 24 hours give any information as to whether I can stop worrying about them or not? How do you know whether skipped/extra beats are benign or not? What kind of chest pain, at rest, is the worrisome kind for someone with severe AS?
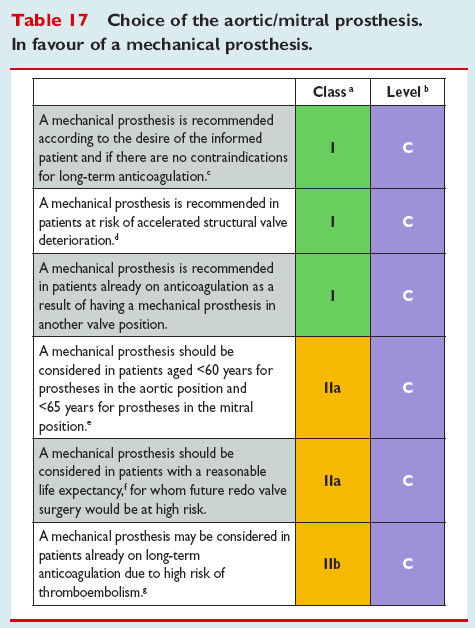
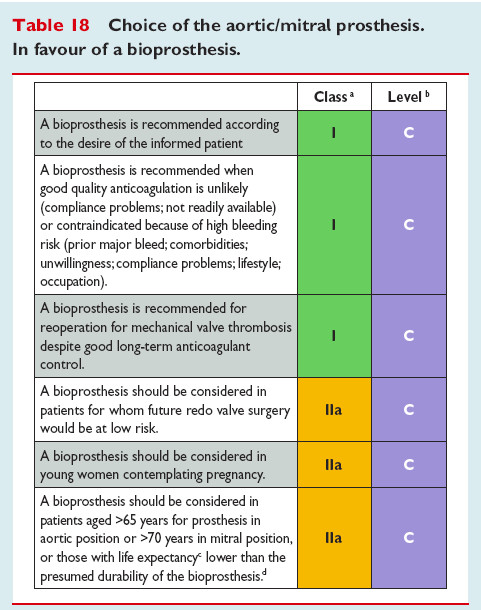
3. Do I really need an "Adults with congenital heart disease" surgeon? There's only like, one of those in my state, from what I can tell, and he, as the doctor put it, 'has a preference for tissue valves' and would not offer me a mechanical one. 'At 40?' I asked. 'Yes'. This leads me to my next question, which is
4. Who are the best surgeons for congenital AVR with a mechanical valve? Can someone recommend a great hospital, in your experience, to have congenital AVR surgery done? How common/safe is minimally invasive surgery (I mean with a smaller incision in the chest, not TAVR) for AVR these days? If it is as safe as a full sternotomy, how can I find a surgeon willing to do this?
5. Should I have a test done beforehand to see if I react badly to Warfarin? What test?
6. I read or heard somewhere that 60% of clinics prohibit patient INR self-testing, presumably for financial reasons (they want you to come in). Um... WHAT??? Should I be concerned about this? I totally want to self manage my INR levels.
7. What INR self-check device is the best, in your experience? Where can I get it?
8. I remember reading about OHS and the menstrual cycle, and how timing could even affect mortality. (!) Has anyone here attempted to time their surgery in this way? If there's anything I can do to offset the higher risk associated with having OHS as a female, I want to do it.
Thank you for reading this far!! Any tips, suggestions, thoughts will be greatly appreciated.
And thank you all so much for teaching me through your posts here, blog posts elsewhere; links, videos and funny pictures shared.... Without you all I would be in full panic mode right now, finding myself living in Arkansas of all places when it's finally time for the surgery.
I have so many questions; and unfortunately am not confident my doctor either can or will answer them. I've learned a lot from the forum already, but now I want to ask a few more specific questions:
1. I went in because I had had chest pain that woke me up from sleep for 5-6 nights in a row. The cardiologist at first said he didn't think it was related to my AS; after viewing the echo he said he thought it WAS... Has anyone else had this? Did it end up being an indication that things were much worse than you thought? (trying to avoid that sudden death thing)
2. I usually deny any symptoms on exertion, (and symptoms at rest that I'd report were always dismissed by cardiologists) though I now think my exercise tolerance must have gradually gotten worse, and with that, shortness of breath walking up hills, etc. With turning 40 I maybe also thought I was just getting old or out of shape... But now I've been told it's time for surgery, that things have progressed/gone downhill, I feel every single pain, ache, twinge and arrhythmia in my heart; along with every episode of gasping for a breath, even at (particularly at) rest. If they are from the AS (which I more and more suspect they must be) - how bad of a sign is this? Would wearing a Holter for 24 hours give any information as to whether I can stop worrying about them or not? How do you know whether skipped/extra beats are benign or not? What kind of chest pain, at rest, is the worrisome kind for someone with severe AS?
3. Do I really need an "Adults with congenital heart disease" surgeon? There's only like, one of those in my state, from what I can tell, and he, as the doctor put it, 'has a preference for tissue valves' and would not offer me a mechanical one. 'At 40?' I asked. 'Yes'. This leads me to my next question, which is
4. Who are the best surgeons for congenital AVR with a mechanical valve? Can someone recommend a great hospital, in your experience, to have congenital AVR surgery done? How common/safe is minimally invasive surgery (I mean with a smaller incision in the chest, not TAVR) for AVR these days? If it is as safe as a full sternotomy, how can I find a surgeon willing to do this?
5. Should I have a test done beforehand to see if I react badly to Warfarin? What test?
6. I read or heard somewhere that 60% of clinics prohibit patient INR self-testing, presumably for financial reasons (they want you to come in). Um... WHAT??? Should I be concerned about this? I totally want to self manage my INR levels.
7. What INR self-check device is the best, in your experience? Where can I get it?
8. I remember reading about OHS and the menstrual cycle, and how timing could even affect mortality. (!) Has anyone here attempted to time their surgery in this way? If there's anything I can do to offset the higher risk associated with having OHS as a female, I want to do it.
Thank you for reading this far!! Any tips, suggestions, thoughts will be greatly appreciated.
And thank you all so much for teaching me through your posts here, blog posts elsewhere; links, videos and funny pictures shared.... Without you all I would be in full panic mode right now, finding myself living in Arkansas of all places when it's finally time for the surgery.





















") Do you use it for sleeping, or just for getting up from sitting, or....?
Do you use it for sleeping, or just for getting up from sitting, or....?
 . I’ll bet there are notes in my file. (“Here’s what I did, this is what I’m doing next week, update the chart. Call me in some 5’s and 1’s. I’ve been at this 30 years. When did you start?”). Okay - I’m more polite then that - but I am comfortable giving input about what I think makes sense for me.
. I’ll bet there are notes in my file. (“Here’s what I did, this is what I’m doing next week, update the chart. Call me in some 5’s and 1’s. I’ve been at this 30 years. When did you start?”). Okay - I’m more polite then that - but I am comfortable giving input about what I think makes sense for me.