Hi
bugchucker;n873679 said:
... I was on coumadin for a few months after my surgery with daily INR monitoring. My levels were all over the place,
firstly please clarify "all over the place" ... also (I know its a long show) but if you have records of the doses as well as the INR I can provide better input.
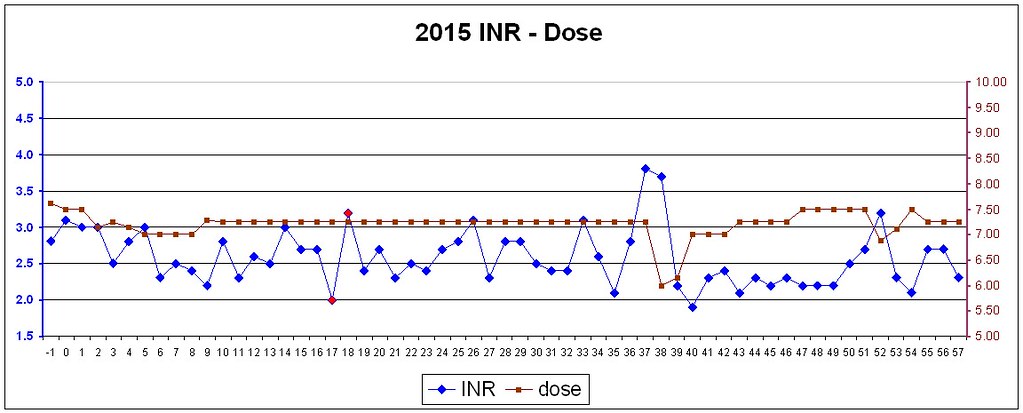
For instance when I show my surgeon (on my meetings with him every year or two) this graph of my results (I have one for every year):
he thinks its an excellent result. So do I
Why because he looks at where the peaks and bottoms are and notes the range ... a clinic manager would have probably made the whole thing worse by attempting to steer every bump and making it just worse. Like watching a kid learn to sail (but clinic managers seem not to learn) and attempting to put rudder input in whenever the bow nods left or right due to swells.
Mostly the worst thing for managing your INR you can do is put your faith in a clinic (which is tragic when you think about it, cos they're the people we should be trusting) as they have dismal records ... for instance most clinics seldom get 80% in range (miserable) yet for the last 5 years I've been > 93% in range ... just going to prove that its not rocket science.
. Are you saying that one could be have a relatively low INR, lower risk of traumatic bleeding and still keep the valve happy? That would certainly make me look again at mechanical more seriously. Thank you for your response.
this graph gets a punding here (cos I cite it about 10% of my posts).
[IMG2=JSON]{"data-align":"none","data-size":"full","src":"https:\/\/c2.staticflickr.com\/4\/3868\/14626794599_c646b1872d_b.jpg"}[/IMG2]
you can see clearly that there is a range between 2 and nearly 5 that the events (either bleed or clot) were very very low. Indeed evidence is emerging from studies that well managed INR (meaning between 2 and 4 > 90% of the time) will give you about the same level of risk for a bleed or a clot as the age related general population.
Feel free to PM me as I'm happy to discuss what I have learned over the years and assist you in self managing (cos if you self manage there are no more arguments with ********* at clinics and you run your own ship). I understand in the GIMP'ed USA that its very difficult to self manage (but not impossible) because the tight collusion with insurance and health providers (to essentially tie in the money to them) makes self management unattractive (cos they don't make money out of it).
Some food for thought from my blog
http://cjeastwd.blogspot.com/2014/09...ng-my-inr.html