Hi
awrigley;n878343 said:
Is there any news on the tests that were being conducted a couple of years ago to lower the INR for Mitral On-X valves? I know that the Aortic On-X valves have had their INR reduced, but have heard nothing more about On-X for Mitral valves.
There has been a study done in Europe (I believe Germany) suggesting that INR for Mitral and aortic can come down a bit lower. They suggested as an outcome of their findings that both Mitral and Aortic position were OK with INR down to 2
Some observations I made from that study:
As > 90% of INR measurements during the entire follow-up period were within the therapeutic range of INR 2.0 to 4.5, which is the lowest erratic INR ever published
[
no wonder there are complications with AC therapy given the variations that occur ... supports weekly testing]
we conclude that low-intensity anticoagulation with a target INR of 2.0 to 3.5 is safe for patients with SJM prostheses in the aortic position as well as the mitral position.
intention-to-treat analysis of two randomized
trials31,32 demonstrated a decrease in bleeding complications without an increase in embolic events with so-called low-dose rather than standard-dose oral anticoagulation.
Reference here:
https://www.ncbi.nlm.nih.gov/pubmed/8269143
if you have diffuculty obtaining the PDF of the report (and you are so inclined to read it yourself), please contact me and I'll send you a copy I have
I am a 57 year old male who had a MVR 8 years ago after endocarditis. My INR still varies wildly, probably because of my "healthy" diet, lots of greens...
Please define wildly? I have been monitoring and self administering my INR for about 4 years now and do not have wildly varying INR since I left being managed by a clinic. I eat quiet irregularly (greens or otherwise) and have extensive notes and readings to back up my views. I'm actually a trained researcher (with a science degree and a science masters degree) and I can say that its common for folks to come to conclusions quickly but that those conclusions aren't aways borne out by a long hard cold look at the data.
I've included below some of my yearly charts of weekly tests so that you can then compare my "typical" INR variations with your own. If you want to try my method of
self management please PM me and we can discuss it. (note: self management, I don't manage you, I teach you to manage you).
[IMG2=JSON]{"data-align":"none","data-size":"full","src":"https:\/\/c2.staticflickr.com\/8\/7682\/16876569857_0ca90610f2_b.jpg"}[/IMG2]
[IMG2=JSON]{"data-align":"none","data-size":"full","src":"https:\/\/c2.staticflickr.com\/2\/1541\/25455579376_2a7ed70af3_b.jpg"}[/IMG2]
[IMG2=JSON]{"data-align":"none","data-size":"full","src":"https:\/\/c1.staticflickr.com\/1\/656\/32000655005_d9aa85c95b_b.jpg"}[/IMG2]
One last point, as per "risk analysis" thinking always keep "the main thing" as
the main thing. In this case the main thing is to minimise harm from INR (being too high or two low). Everything else is just secondary. So don't try to consider "low dose" consider keeping your INR both reasonably stable and every medical professional )who knows their arse from their head) that I've shown my INR results to calls my results "very stable". So don't try to shoot for a flat line because that's not the main goal.
All the evidence we have so far (from what, 50 years of intensive research on Warfarin) suggests that if you keep your INR within bounds that you will have scarcely more than the age related incidence of clot or bleed related events. Remember that as one ages, the general population has increased risk of stroke or bleed anyway.
There is a tendency for people to focus on "reducing their dose" ... which is a nonsense which has absolutely no basis in any evidence. So don't think in terms of "reduced dose" think in terms of "being in range.
What is range? Well, I'll leave you with this:
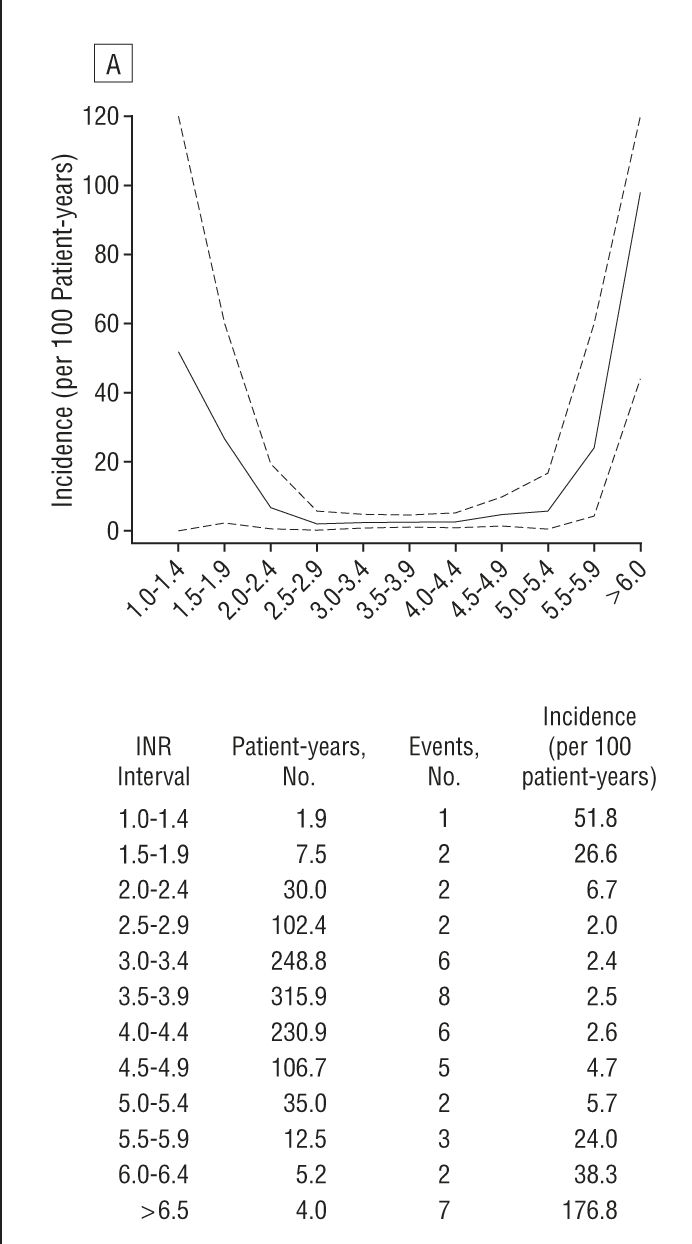
from "Optimal level of oral anticoagulant therapy for the prevention of arterial thrombosis in patients with mechanical heart valve prostheses, atrial fibrillation, or myocardial infarction: a prospective study of 4202 patients."
jamanetwork.com/journals/jamainternalmedicine/fullarticle...
note the flat point that is very low incidence between INR = 2 and INR = 5 ... that my friend is your safety zone.
Myself I steer towards 2.5 (if low, steer higher, if high steer lower) and use that data to know that if my INR should spike to 5 (it has never) then I'm not going to stress about it and just manage it back to 2.5
Best Wishes