pellicle
Professional Dingbat, Guru and Merkintologist
for anyone who does self management (or is thinking of it)

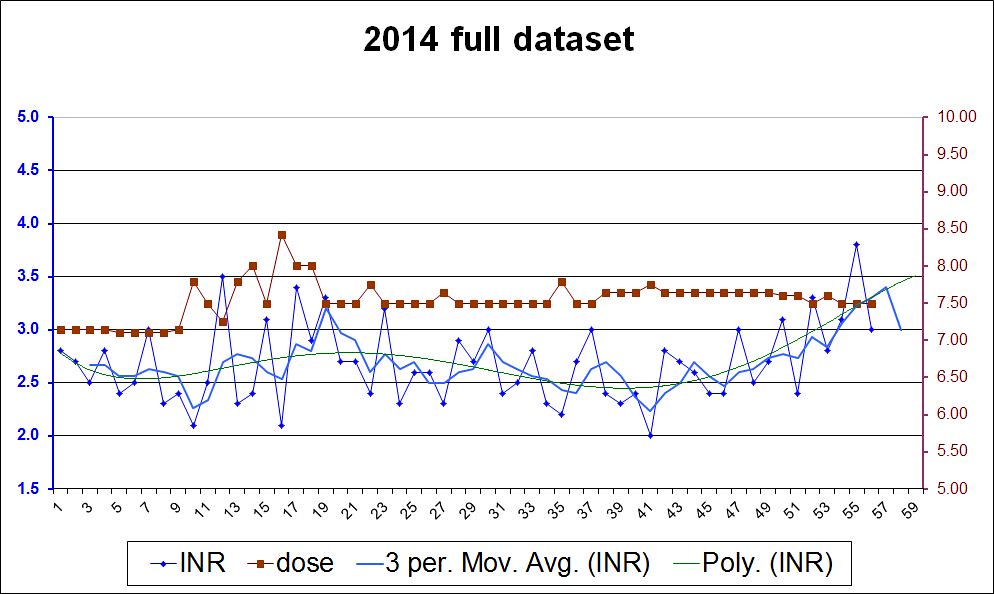
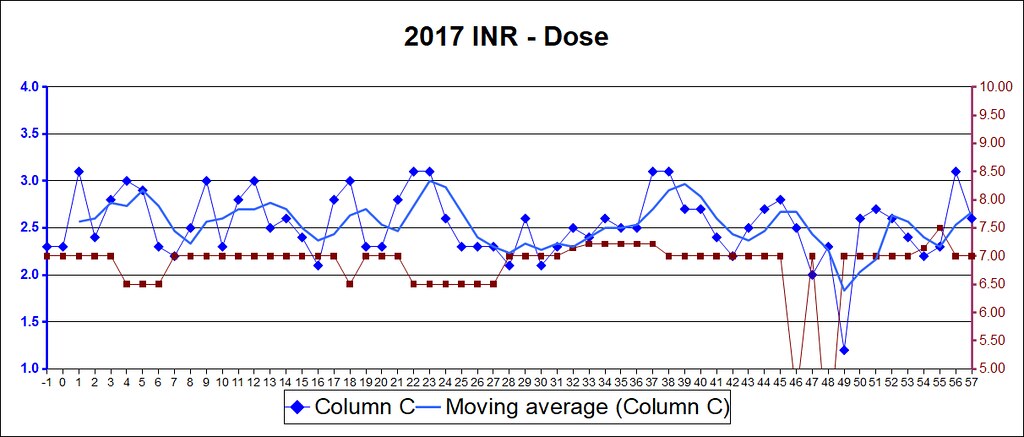
you can clearly see when I had my small surgery.
Happy New Year self managers
| INR | Warfarin (daily mg) | |
|---|---|---|
average | 2.6 | 7.0516 |
std dev | 0.3 | 0.3 |
max | 3.4 | 7.5 |
min | 1.5 | 6.0 |
over event | 1 | |
under event | 1 | |
inRange % | 96.4 | |
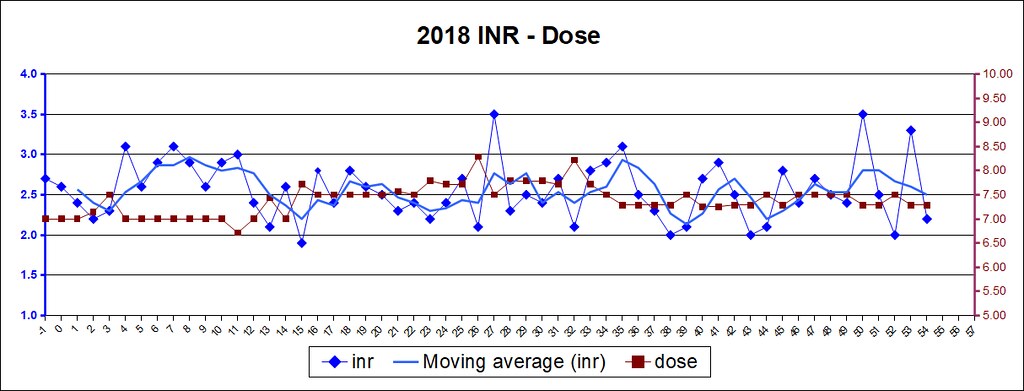
you can clearly see when I had my small surgery.
Happy New Year self managers
 (Suppose I should add that)
(Suppose I should add that)
 Do you eat and drink the same things, for the most part? I find that I'm so afraid of being in the twos, I tend to shoot for 3 and end up hitting 4.
Do you eat and drink the same things, for the most part? I find that I'm so afraid of being in the twos, I tend to shoot for 3 and end up hitting 4.