


@Daniel758 It's good to read normal people who think normally, without any disturbances. I am absolutely sure that many of you here do not write to avoid problems with these people. Time is too precious to spend with fanatic people.
@dick0236 Even though they deleted my post, I still don't believe that your valve is 56 years old and you are 90 years old. Sorry, I don't believe it.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10493300/
Regards...
@dick0236 Even though they deleted my post, I still don't believe that your valve is 56 years old and you are 90 years old. Sorry, I don't believe it.
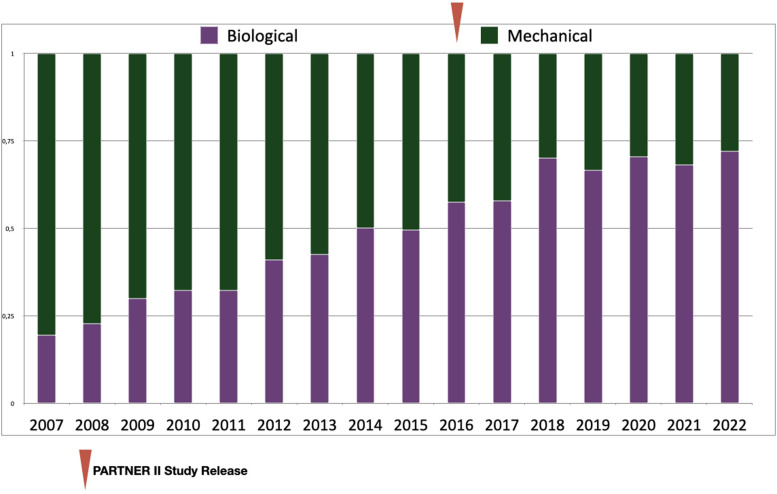
Currently, despite continued issues with durability (1), biological prosthetic valves are increasingly chosen over mechanical valves for surgical aortic valve replacement (SAVR) in adult patients of all ages, at least in Western countries. For younger patients, this choice means assuming the risks associated with a redo SAVR or valve-in-valve procedure.
Mechanical prosthetic valves (MPVs), for which oral direct Factor Xa inhibitors failed to be a valid option (2, 3), are not generally considered in patients above 65 years-old, even if a long-standing anticoagulant therapy is required and despite the fact that acceptable outcomes with a MPV may be achieved in selected elderly patients (4). To avoid imposing to a young patient a life-long anticoagulant therapy whenever a Ross procedure or an aortic valvular repair is out of reach, a BPV in aortic position is often perceived to be the best second choice. Thus, in Western countries and despite consensus recommendations (5–7), BPVs are nowadays implanted in a significant proportion of young and middle-aged patients requiring SAVR (8) therefore assuming the risks associated with a subsequent redo SAVR or with a valve-in-valve trans catheter aortic valve replacement (ViV-TAVR). Concerning TAVR, lowering the age-threshold and extending indications towards low-risk patients will further amplify this global move towards BPV with an exponential rise (9).
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10493300/
Regards...




















